
Buccal fat removal, also called buccal lipectomy or cheek reduction, is an elective cosmetic surgery that removes part or all of the buccal fat pad in the lower cheek to create a slimmer, more contoured lower face and emphasize the cheekbones.
What is buccal fat removal?
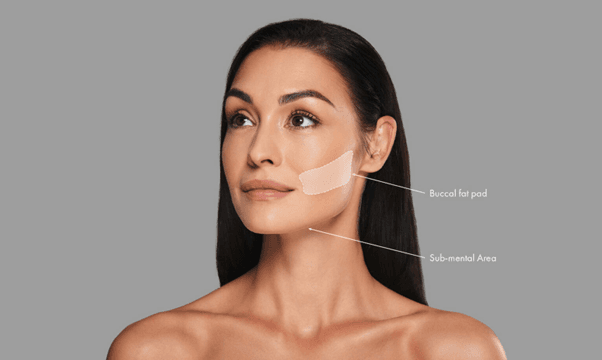
Buccal fat removal, also called buccal lipectomy, is a cosmetic surgical procedure that reduces prominence in the lower cheeks by removing part or all of the buccal fat pads—discrete pockets of deep facial fat located between the cheekbone and lower jaw. The goal is to create a slimmer, more contoured midface and to emphasize cheekbone definition, producing what many describe as a more sculpted or refined facial silhouette. The operation is most often performed through small intraoral incisions inside the mouth to avoid external scars, under local anesthesia with sedation or general anesthesia depending on the surgeon and patient preference. During the procedure the surgeon gently exposes the buccal fat pad, teases out an appropriate volume tailored to the individual’s facial anatomy and aesthetic goals, and trims or removes it while protecting facial nerves and salivary ducts. Recovery is generally quick, with short-term swelling, mild discomfort, and a brief period of dietary modification to protect the incision sites. Because facial aging and future weight changes can alter cheek fullness, careful patient selection and realistic expectations are essential; buccal fat removal suits those seeking permanent reduction of cheek fullness but may not be appropriate for individuals prone to facial volume loss with age.

Who is a good candidate for buccal fat removal?
A good candidate for buccal fat removal is an adult in overall good health who has persistent fullness of the lower cheeks that does not meaningfully change with weight loss and who desires a slimmer, more contoured midface; ideal candidates typically have a fuller, rounded facial shape with distinct buccal fat pad prominence and enough remaining facial soft tissue to avoid an overly gaunt appearance later in life. Candidates should have realistic expectations about the procedure’s permanent nature and how aging, future weight loss, or facial fat redistribution may alter long‑term results. People with significant skin laxity, very thin faces, or a strong tendency toward age‑related facial volume loss are generally poor candidates because removal can accentuate hollows as aging progresses. Good candidates are nonsmokers or willing to stop smoking before and after surgery, have no uncontrolled medical conditions that impair healing, and demonstrate good oral hygiene if intraoral incisions will be used. Psychological readiness and clear aesthetic goals are important; a thorough consultation with a board‑certified plastic surgeon or facial specialist includes facial analysis, discussion of alternatives (such as fillers, fat grafting, or buccal lipectomy combined with other procedures), and a personalized plan that balances immediate contour improvements with long‑term facial harmony.

How is Buccal Fat Removal Procedure done?
Buccal fat removal is usually performed under local anesthesia with sedation or general anesthesia depending on patient preference and surgeon recommendation; after marking and sterile preparation, the surgeon makes a small incision on the inside of the cheek, typically above the upper molars, to avoid any external scar. Through this intraoral opening the buccal fat pad is gently exposed by blunt dissection and the surgeon teases out an appropriate portion of the fat, tailoring the volume removed to the patient’s anatomy and aesthetic goals while taking care to protect the facial nerve branches and Stensen’s duct. The excised fat is trimmed and removed, and the pocket is inspected for hemostasis before the mucosal incision is closed with dissolvable sutures. In select cases an external approach or combined procedures (for example, rhytidectomy or chin augmentation) may be used to achieve better overall facial balance. The procedure is typically brief, often under an hour, and patients receive perioperative instructions on oral care, diet modification, activity restriction, and signs of complications to watch for. Follow‑up visits allow the surgeon to monitor healing, manage swelling, and ensure a natural, symmetric contour as tissue settles.
What are the risks associated with buccal fat removal surgery?
Buccal fat removal is generally safe when performed by an experienced surgeon, but it carries specific risks patients should consider.
Early complications include bleeding, infection, and poor wound healing at the intraoral incision site, which can cause pain, prolonged swelling, or scarring inside the mouth.
Temporary numbness or altered sensation may occur from nerve irritation; although usually transient, partial or persistent sensory changes are possible.
Asymmetry or uneven fat removal can produce visible contour irregularities that sometimes require revision.
Over‑resection is a distinct long‑term risk: removing too much buccal fat can lead to an overly hollowed or gaunt appearance as natural aging and future weight loss reduce facial volume, a change that is difficult to reverse.
Injury to nearby structures such as the parotid (Stensen’s) duct or facial nerve branches is rare but can cause chronic dryness, salivary fistula, or motor weakness.
Excessive scar tissue or adhesions inside the cheek may restrict movement or cause discomfort. Swelling and numbness can mask early problems, delaying diagnosis of complications.
Smoking, poor oral hygiene, and uncontrolled medical conditions increase the chance of adverse outcomes. A careful preoperative assessment, conservative fat removal, and clear discussion of aesthetic risks help minimize complications and align expectations.

What is the recovery time for buccal fat removal surgery?
Recovery from buccal fat removal is generally quick but occurs in stages: the first 48 to 72 hours bring the most swelling and possible bruising, which respond to cold compresses, head elevation, and prescribed pain control. Most patients can resume light, nonstrenuous work within three to seven days, though individual comfort varies. Oral soreness and mild difficulty opening the mouth or chewing are common for several days, so a soft diet is usually recommended for the first few days to a week. Bruising typically fades within one to two weeks while residual swelling can take several weeks to noticeably subside. Numbness or altered sensation inside the cheek often improves over weeks to months. Strenuous exercise, heavy lifting, and activities that strain the face should be avoided for two to four weeks to reduce bleeding risk and swelling. Final contour and subtle refinement continue to develop as tissues settle over three to six months, at which point long‑term results are clearer. Smokers, people with healing problems, or those who experience infection or asymmetry may have prolonged recovery or need revision.

Conclusion
Buccal fat removal can provide a lasting, more sculpted midface for carefully selected patients, but success depends on conservative surgical planning, realistic expectations, and awareness that aging and weight changes may alter long‑term results; discussing goals and risks with an experienced facial surgeon ensures the best chance of a natural, balanced outcome.
Read More