
Penis enlargement, also called penile augmentation, refers to medical and cosmetic interventions intended to increase visible length, girth, or both.
What is penis enlargement surgery?
Penis enlargement surgery, often called penile augmentation or phalloplasty, encompasses a range of procedures designed to change the penis’s visible length, circumference, or appearance rather than to treat a medical dysfunction; most candidates seek surgery for aesthetic or psychological reasons rather than for functional necessity. Common lengthening techniques include division of the suspensory ligament to allow more of the penile shaft to hang outside the body, sometimes combined with skin rearrangement or grafts to prevent retraction; however, ligament release typically increases flaccid length more than erect length and may require postoperative traction to maintain gains. Girth enhancement methods include autologous fat transfer, dermal grafts, injectable fillers (e.g., hyaluronic acid), or synthetic implants, each with tradeoffs in durability, feel, and complication risk. Some comprehensive approaches borrow from reconstructive urology and plastic surgery, using complex grafting or implant techniques for more dramatic changes. All procedures carry risks: infection, scarring, loss of sensation, erectile dysfunction, penile curvature, asymmetry, resorption of grafted material, and unsatisfactory cosmetic results; in some cases, surgery can paradoxically shorten erect length or impair function. Because many people seeking augmentation have normal anatomy, psychological assessment and realistic expectations are critical, and non‑surgical alternatives (vacuum devices, traction therapy, counseling) may be safer or more appropriate for some individuals.

Who may need or want to have penis enlargement surgery?
Men who consider penis enlargement surgery typically fall into several groups. Some seek treatment because of persistent perceived inadequacy about size that affects self‑esteem, sexual confidence, or intimate relationships despite having normal anatomy; these concerns are often psychological rather than medical. Others have congenital conditions such as micropenis or developmental anomalies that make reconstruction or augmentation medically appropriate. Men with post‑traumatic deformities, scarring from prior surgery, or complications from penile cancer treatment may pursue augmentation as part of reconstructive care. A smaller group seeks correction after penile shortening following procedures like radical prostatectomy or Peyronie’s disease surgery. Candidates may also include men whose apparent penile length is reduced by excess pubic fat or obesity, where weight loss or liposuction can sometimes be a simpler first step. Good candidates are those with realistic expectations, stable mental health, and clear understanding of risks, alternatives, and likely outcomes; surgeons typically screen for body image disorders and recommend counseling when appropriate. Because many procedures are cosmetic and carry risks such as infection, scarring, and functional changes, careful evaluation by a board‑certified urologist or plastic surgeon experienced in penile procedures is essential before deciding on surgery and to explore non‑surgical alternatives first when appropriate too.

What are the Penis Enlargement Methods?
Penis enlargement encompasses several distinct approaches aimed at increasing visible length, circumference, or the apparent size by reducing surrounding tissue.
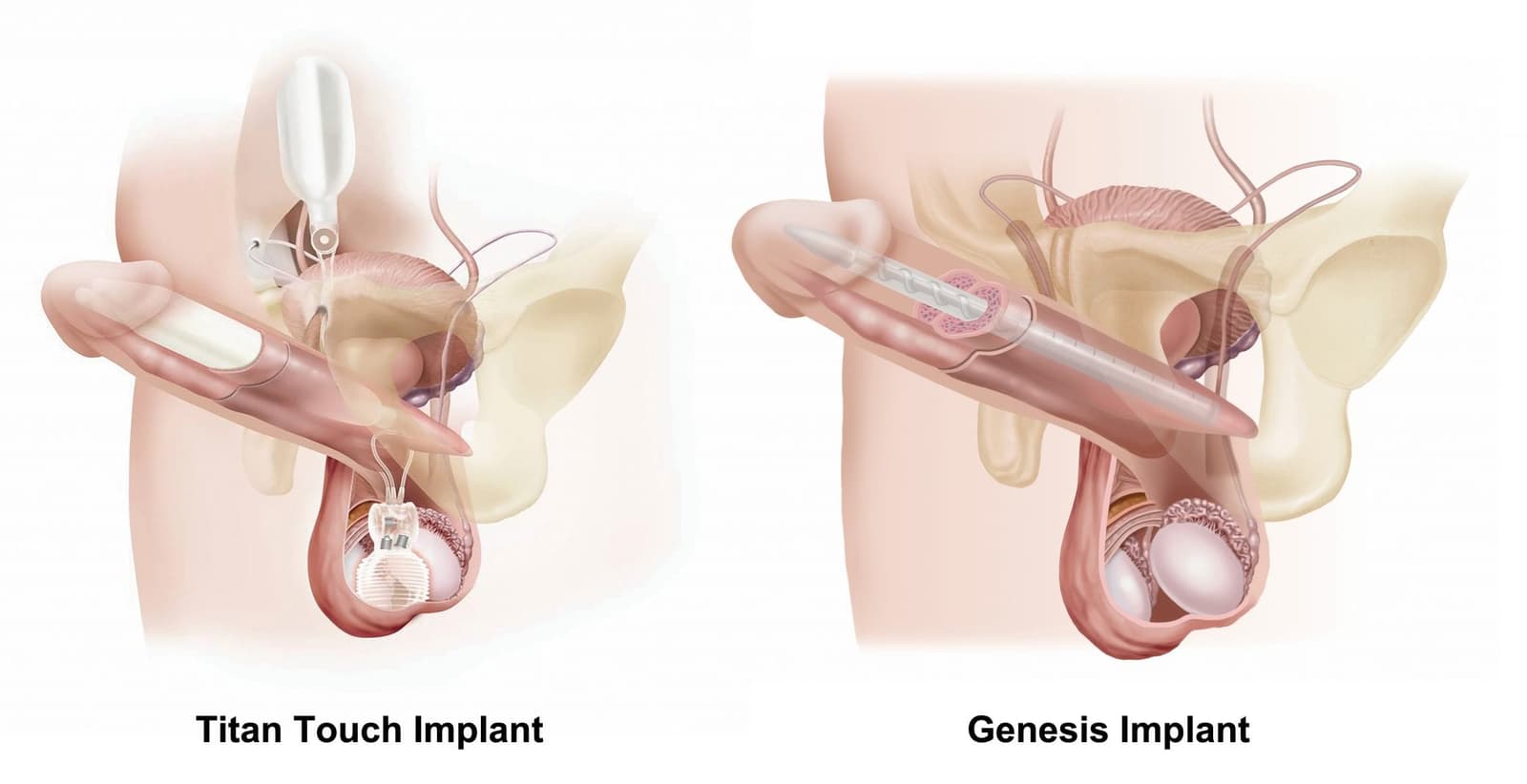
Surgical enlargement typically involves ligamentolysis (division of the suspensory ligament) to increase flaccid visible length, sometimes combined with skin rearrangement or insertion of spacers, and girth augmentation using autologous fat transfer, dermal grafts, or synthetic implants such as the Penuma device; outcomes vary and some techniques may change sensation or erectile function.
Pubic fat removal (suprapubic liposuction) is a less invasive adjunct or standalone option that reduces the fat pad above the penis so more shaft is exposed, often producing a noticeable cosmetic gain without altering penile tissue itself; it is commonly recommended when excess pubic adiposity is the main contributor to perceived shortness.
Penis thickening strategies focus on increasing circumference and include fat grafting (autologous fat), injectable fillers (e.g., hyaluronic acid), and dermal or synthetic grafts; fat can resorb unpredictably and fillers may require repeat treatments, while grafts and implants carry surgical risks and potential for irregularities or infection.
Across methods, common risks include infection, scarring, asymmetry, loss of sensation, erectile dysfunction, and unsatisfactory cosmetic results; some procedures can paradoxically shorten erect length or create functional problems if complications occur. Because many candidates have normal anatomy and seek cosmetic change, psychological screening, realistic expectations, and choosing a board‑certified urologist or plastic surgeon experienced in penile procedures are critical; non‑surgical alternatives (traction devices, vacuum therapy, weight loss for pubic fat) may be safer first steps for some men.

What happens during penis enlargement procedures?
During a typical penis enlargement pathway, the process begins with a comprehensive consultation where a surgeon or urologist assesses anatomy, medical history, and expectations, screens for body image disorders, and discusses realistic outcomes and risks.
For surgical lengthening, the operation usually takes place under general or regional anesthesia; the surgeon performs suspensory ligament release (ligamentolysis) to allow more of the penile shaft to hang outside the pubic bone, often combined with skin rearrangement or placement of spacers to reduce retraction, and may recommend postoperative traction to help maintain gains.
Girth augmentation can be done surgically by harvesting autologous fat for grafting, inserting dermal grafts, or placing synthetic implants; each technique involves incisions, tissue manipulation, and careful shaping to try to achieve a natural contour, but fat grafts can resorb unpredictably and implants carry infection and extrusion risks.
Less invasive options are performed either in clinic or minor‑procedure settings: suprapubic liposuction removes excess pubic fat to expose more shaft and is often combined with other procedures or used alone when a fat pad is the main issue; injectable fillers such as hyaluronic acid can increase girth temporarily and are done under local anesthesia but may require repeat treatments and can cause lumps or unevenness.
Across all methods, intraoperative steps include sterile preparation, precise tissue handling to preserve neurovascular structures, and hemostasis; surgeons typically place drains or dressings as needed and provide detailed postoperative instructions.

What are the risks or complications of penis enlargement procedures?
Penis enlargement interventions—whether surgical lengthening, girth augmentation, injectable fillers, or adjunctive measures like suprapubic liposuction—are associated with a range of medical, functional, and aesthetic complications that patients should understand before proceeding.
Infection and wound healing problems can occur after any invasive procedure and may lead to abscess, prolonged antibiotics, or revision surgery; scarring and adhesions can distort penile contour or tether the shaft, producing cosmetic irregularities.
Procedures that manipulate tissue risk sensory changes, including numbness or hypersensitivity of the glans or shaft, which can be temporary or permanent and may affect sexual satisfaction.
Some techniques carry a measurable risk of erectile dysfunction or vascular injury, either from direct nerve or vessel trauma or from postoperative fibrosis.
Girth augmentation using autologous fat is unpredictable because fat resorption can reduce the initial gain and create unevenness or lumps, while synthetic implants or grafts risk extrusion, infection, or chronic foreign‑body reactions.
Lengthening operations can paradoxically reduce erect length or produce penile instability if the suspensory support is altered without adequate reconstruction, and any procedure can result in asymmetry, curvature, or unsatisfactory cosmetic outcome that may require corrective surgery.
Beyond physical harms, there is a significant psychological risk: many candidates have normal anatomy and may experience persistent dissatisfaction, body‑image distress, or regret after surgery.
Recovery also involves downtime, activity restrictions, and potential need for repeat procedures, all of which carry cost and health implications.
Recovery after penis enlargement surgery
Recovery after penis enlargement varies by technique but follows common phases: immediate postoperative swelling and bruising, managed with dressings, cold packs, prescribed pain medication, and often a short course of antibiotics; patients are advised to rest, sleep on their back, and avoid strenuous activity for the first 1–2 weeks. Early follow‑up visits check wounds and remove sutures or drains, and surgeons may recommend compression or support garments to shape grafts or reduce edema. Sexual activity is typically restricted for 2–6 weeks depending on the procedure, with fuller healing and tissue remodeling continuing for months; temporary changes in appearance (shorter or distorted look while swelling peaks) are common before gradual improvement. Specific timelines differ: injectable fillers and implants often show assessable results by 6–12 weeks, while fat grafting and major surgical reconstructions may take 3–6 months or longer for final contour as grafts settle and scar tissue matures. Patients should watch for red flags—fever, increasing pain, wound drainage, or signs of vascular compromise—and contact their surgeon promptly. Adherence to postoperative instructions, realistic expectations, and scheduled follow‑ups improve outcomes and help manage complications such as asymmetry, graft resorption, or sensory changes.

Conclusion
Penis enlargement surgery can offer cosmetic change for some men but carries meaningful medical, functional, and psychological risks; careful evaluation, realistic expectations, and choosing an experienced, board‑certified specialist are essential before proceeding.
Read More